Masimo and University Hospitals Partner to Combat Nurse Burnout

Masimo Patient SafetyNet™ Remote Monitoring and Supplemental Alarm System Improves Nursing Workflow and Reduces Nursing Workloads
IRVINE, Calif.–(BUSINESS WIRE)–Masimo (NASDAQ: MASI) today announced that University Hospitals (UH) of Cleveland is using Masimo Patient SafetyNet™, a remote monitoring and supplemental alarm system, to combat nurse burnout by improving workflows and reducing workloads. As the COVID-19 pandemic continues to strain healthcare infrastructure around the world, hospitals are dealing with higher than usual rates of nurse turnover. Patient SafetyNet offers a technological approach to supporting nursing workflows, as both UH’s experience and clinical evidence have shown.
![]()
During the pandemic, more than 80% of hospitals have reported an increase in nurse turnover.1 In a survey of more than 20,000 nurses conducted in 2020, 18% intended to resign, 50% responded that work was negatively impacting their health, and 47% reported that insufficient staffing contributed to their desire to leave the profession.2 Nurse staffing shortages have been associated with both increased costs and, crucially, decreased patient safety: A survey of 138 facilities covering more than 120,000 nurses found that the average cost of turnover ranged from $37,400 to $58,400 per nurse.3 And an observational, retrospective study of almost 200,000 patients across 43 hospital units found a significant association between increased patient mortality and nurse staffing below target levels.4
In a newly released testimonial, available here, UH – one of the largest health systems in Ohio – shows how their experience with continuous remote monitoring using Patient SafetyNet, is positively impacting their nursing practices and the quality of care nurses are able to provide while improving efficiency and staff satisfaction. Within three weeks of implementing Patient SafetyNet, for example, UH found that the average time between obtaining a patient’s vital signs at the point of care and documenting them in the electronic medical record (EMR) had decreased from more than 60 minutes to less than 5 minutes, resulting in a time savings of one FTE per shift.
UH first implemented Patient SafetyNet in 2016 following an incident in which an unnoticed, rapid deterioration in a patient’s condition resulted in emergency resuscitation and ICU transfer. Jenna Zarack, a nurse at UH’s Geauga Medical Center, said that Patient SafetyNet is “a great way to protect patients; it’s a great way to protect nurses, and for nurses to be able to help their patients in a fast, immediate response, so we don’t get to a code, we don’t get to a rapid response situation.” Sara Knowles, MSN, Clinical Nurse Specialist at UH, added, “The technology allows us to have eyes on our patients 24/7, which has proven especially valuable during our nursing shortage and the global pandemic.”
When asked why UH is now planning to expand use of Patient SafetyNet – which is already in use in 8 med-surg units across 5 UH hospitals – Michelle Hereford, UH’s Chief Nursing Executive, explained, “We’ve found that Patient SafetyNet’s continuous surveillance monitoring and automation capabilities help lower the burden on nurses and support them in providing quality care for every patient and catching potential patient deterioration before it’s too late. Coupled with the improvements we’ve seen in efficiency, staff confidence, and staff satisfaction since installing the system, expanding use of Patient SafetyNet is frankly a no-brainer.”
In addition to the experiences of Patient SafetyNet users like UH, there is significant clinical evidence for the efficiency and workflow benefits the centralized surveillance monitoring system offers, such as:
- In a recent study published in the Journal of PeriAnesthesia Nursing researchers evaluated the utility and impact of Patient SafetyNet by surveying nurses before and after implementation and found that use of the system decreased the number of physical assessments, resulting in a reduction in nursing workload, and also recommended the use of continuous respiratory rate and oxygen saturation monitoring (which was implemented as part of the system) after general anesthesia, for patients’ safety.5
- In a study conducted at Dartmouth-Hitchcock Medical Center, researchers investigated the impact of Patient SafetyNet on clinical workflow, and found a significant decrease in the time required to obtain and record vital signs (with mean assessment time dropping from 179 seconds to 129 seconds, saving an average of 3 hours a day in a 36-bed unit). They also found a significantly higher rate of patient data being accurately filled out in electronic medical records (EMRs), and an overall “very high” staff satisfaction rate with the system. The researchers concluded, “The enhanced monitoring system received high staff satisfaction ratings and significantly improved key clinical elements related to early recognition of changes in patient state, including reducing average vital signs data collection time by 28%, increasing patient monitoring time (rate ratio 1.22), and availability and accuracy of patient information.”6
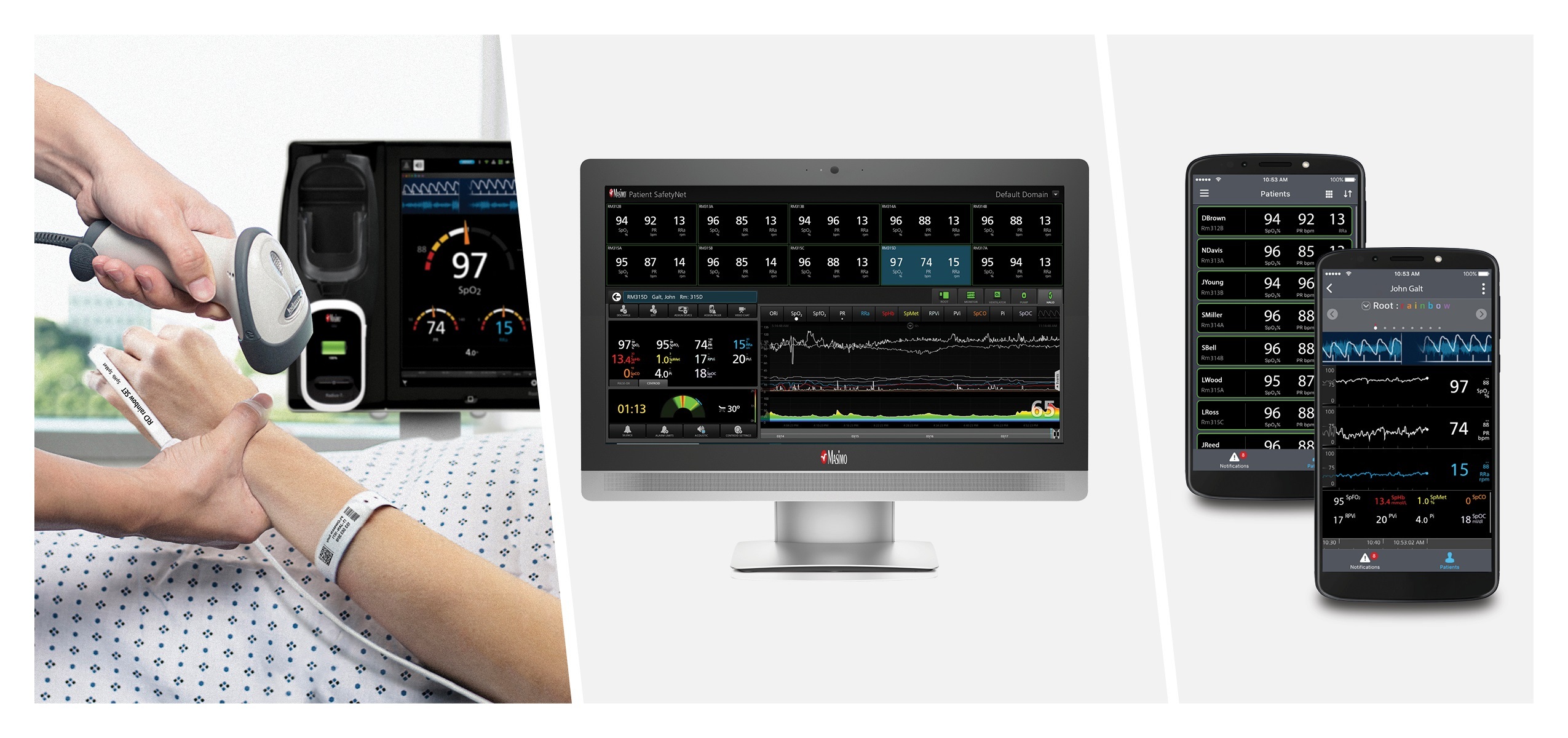
Patient SafetyNet, powered by the Masimo Hospital Automation™ platform, displays real-time information from connected Masimo and third-party devices at central stations and on remote smart devices using Replica™, helping clinicians keep track of up to 200 patients per view station at a time. In addition, the system allows actionable alarms and alerts to be sent directly to clinicians, regardless of their location. Automatic escalation is provided for unattended alarms, helping to facilitate better awareness when patients need assistance. In addition to the workflow and workload reductions it offers, use of Patient SafetyNet for continuous remote supplemental monitoring with Masimo SET® pulse oximetry has been shown to have a significant impact on patient outcomes. For example, in multiple studies conducted over ten years at Dartmouth-Hitchcock, researchers found dramatic reductions in rapid response rescue events, ICU transfers, and zero deaths or preventable brain damage due to opioids in monitored patients.7-9
In addition to its powerful connectivity and automation features, which drive improvements for patients and nurses alike, Patient SafetyNet also offers powerful, integrated data aggregation and reporting software, Iris® Analytics. Designed to transform patient data into actionable information on hospital performance, floor protocol, and individual patient progress, Iris Analytics allows users to analyze past alarm events, notifications, and much more, to gain insight into their institution’s performance—and model improvements to support the reduction of nuisance alarms and thus improve workflows. Based on analysis of even just one to two weeks of past alarm event data, the Limit Analysis Report helps clinicians simulate alarm scenarios using theoretical alarm thresholds and delays, providing key data to help them evaluate and refine their alarm strategies to better meet their needs.
UH Chief Clinical Transformation Officer, Peter Pronovost, MD, commented, “Masimo Patient SafetyNet has been a valuable component in advancing our Zero Harm initiative within the University Hospitals system. It’s allowed us to increase the efficiency of our caregivers, reduce clinical errors, and help us focus on the timely delivery of compassionate care to our patients. It has also been a critical monitoring partner during the pandemic, when the condition of our COVID patients can dramatically change.”
Joe Kiani, Founder and CEO of Masimo, said, “As the pandemic continues, hospitals and other healthcare facilities are coming up against resource limitations across the board – from equipment, supplies, and beds to doctors and administrative staff – but the shortage of qualified nurses, due to burnout, may be the most significant challenge of all. Masimo has spent more than 25 years improving monitoring and automation technologies designed not only to improve patient outcomes and reduce the cost of care, but to make it easier for nurses to do their jobs effectively and efficiently. We hope that more and more institutions, like University Hospitals, will have the opportunity to experience the benefits that Patient SafetyNet can provide for patients and staff alike.”
@Masimo | #Masimo
About Masimo
Masimo (NASDAQ: MASI) is a global medical technology company that develops and produces a wide array of industry-leading monitoring technologies, including innovative measurements, sensors, patient monitors, and automation and connectivity solutions. Our mission is to improve patient outcomes, reduce the cost of care, and take noninvasive monitoring to new sites and applications. Masimo SET® Measure-through Motion and Low Perfusion™ pulse oximetry, introduced in 1995, has been shown in over 100 independent and objective studies to outperform other pulse oximetry technologies.11 Masimo SET® has also been shown to help clinicians reduce severe retinopathy of prematurity in neonates,12 improve CCHD screening in newborns,13 and, when used for continuous monitoring with Masimo Patient SafetyNet™ in post-surgical wards, reduce rapid response team activations, ICU transfers, and costs.6-9 Masimo SET® is estimated to be used on more than 200 million patients in leading hospitals and other healthcare settings around the world,14 and is the primary pulse oximetry at 9 of the top 10 hospitals as ranked in the 2021-22 U.S. News and World Report Best Hospitals Honor Roll.15 Masimo continues to refine SET® and in 2018, announced that SpO2 accuracy on RD SET® sensors during conditions of motion has been significantly improved, providing clinicians with even greater confidence that the SpO2 values they rely on accurately reflect a patient’s physiological status. In 2005, Masimo introduced rainbow® Pulse CO-Oximetry technology, allowing noninvasive and continuous monitoring of blood constituents that previously could only be measured invasively, including total hemoglobin (SpHb®), oxygen content (SpOC™), carboxyhemoglobin (SpCO®), methemoglobin (SpMet®), Pleth Variability Index (PVi®), RPVi™ (rainbow® PVi), and Oxygen Reserve Index (ORi™). In 2013, Masimo introduced the Root® Patient Monitoring and Connectivity Platform, built from the ground up to be as flexible and expandable as possible to facilitate the addition of other Masimo and third-party monitoring technologies; key Masimo additions include Next Generation SedLine® Brain Function Monitoring, O3® Regional Oximetry, and ISA™ Capnography with NomoLine® sampling lines. Masimo’s family of continuous and spot-check monitoring Pulse CO-Oximeters® includes devices designed for use in a variety of clinical and non-clinical scenarios, including tetherless, wearable technology, such as Radius-7® and Radius PPG™, portable devices like Rad-67®, fingertip pulse oximeters like MightySat® Rx, and devices available for use both in the hospital and at home, such as Rad-97®. Masimo hospital automation and connectivity solutions are centered around the Masimo Hospital Automation™ platform, and include Iris® Gateway, iSirona™, Patient SafetyNet, Replica™, Halo ION™, UniView®, UniView :60™, and Masimo SafetyNet™. Additional information about Masimo and its products may be found at www.masimo.com. Published clinical studies on Masimo products can be found at www.masimo.com/evidence/featured-studies/feature/.
ORi and RPVi have not received FDA 510(k) clearance and are not available for sale in the United States. The use of the trademark Patient SafetyNet is under license from University HealthSystem Consortium.
References
- https://www.incrediblehealth.com/blog/study-covid-19-anniversary-nurse-impact/
- https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/year-one-covid-19-impact-assessment-survey/
- https://rnbsnonline.unm.edu/articles/high-cost-of-nurse-turnover.aspx
- Needleman J, Buerhaus P, Pankratz VS, Leibson CL, Stevens SR, Harris M. Nurse staffing and inpatient hospital mortality. N Engl J Med. 2011 Mar 17;364(11):1037-45. doi: 10.1056/NEJMsa1001025. PMID: 21410372.
- Ishikawa M, Sakamoto A. Patient SafetyNet for the Evaluation of Postoperative Respiratory Status by Nurses: A Presurvey and Postsurvey Study. J PeriAnesth Nursing. DOI: https://doi.org/10.1016/j.jopan.2020.03.005.
- McGrath S, Perreard I, Garland M, Converse K, and Mackenzie T. Improving patient safety and clinician workflow in the general care setting with enhanced surveillance monitoring. J Biomed Health Infor. DOI 10.1109/JBHI.2018.2834863.
- Taenzer A et al. Impact of pulse oximetry surveillance on rescue events and intensive care unit transfers: a before-and-after concurrence study. Anesthesiology. 2010:112(2):282-287.
- Taenzer A et al. Postoperative Monitoring – The Dartmouth Experience. Anesthesia Patient Safety Foundation Newsletter. Spring-Summer 2012.
- McGrath S et al. Surveillance Monitoring Management for General Care Units: Strategy, Design, and Implementation. The Joint Commission Journal on Quality and Patient Safety. 2016 Jul;42(7):293-302.
- McGrath S et al. Inpatient Respiratory Arrest Associated With Sedative and Analgesic Medications: Impact of Continuous Monitoring on Patient Mortality and Severe Morbidity. J Patient Saf. 2020 14 Mar. DOI: 10.1097/PTS.0000000000000696.
- Published clinical studies on pulse oximetry and the benefits of Masimo SET® can be found on our website at http://www.masimo.com. Comparative studies include independent and objective studies which are comprised of abstracts presented at scientific meetings and peer-reviewed journal articles.
- Castillo A et al. Prevention of Retinopathy of Prematurity in Preterm Infants through Changes in Clinical Practice and SpO2 Technology. Acta Paediatr. 2011 Feb;100(2):188-92.
- de-Wahl Granelli A et al. Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: a Swedish prospective screening study in 39,821 newborns. BMJ. 2009;Jan 8;338.
- Estimate: Masimo data on file.
- http://health.usnews.com/health-care/best-hospitals/articles/best-hospitals-honor-roll-and-overview.
About University Hospitals / Cleveland, Ohio
Founded in 1866, University Hospitals serves the needs of patients through an integrated network of 23 hospitals (including 5 joint ventures), more than 50 health centers and outpatient facilities, and over 200 physician offices in 16 counties throughout northern Ohio. The system’s flagship quaternary care, academic medical center, University Hospitals Cleveland Medical Center, is affiliated with Case Western Reserve University School of Medicine, Oxford University and the Technion Israel Institute of Technology. The main campus also includes the UH Rainbow Babies & Children’s Hospital, ranked among the top children’s hospitals in the nation; UH MacDonald Women’s Hospital, Ohio’s only hospital for women; and UH Seidman Cancer Center, part of the NCI-designated Case Comprehensive Cancer Center. UH is home to some of the most prestigious clinical and research programs in the nation, with more than 3,000 active clinical trials and research studies underway. UH Cleveland Medical Center is perennially among the highest performers in national ranking surveys, including “America’s Best Hospitals” from U.S. News & World Report. UH is also home to 19 Clinical Care Delivery and Research Institutes. UH is one of the largest employers in Northeast Ohio with more than 30,000 employees. Follow UH on LinkedIn, Facebook and Twitter. For more information, visit UHhospitals.org.
Forward-Looking Statements – Masimo
This press release includes forward-looking statements as defined in Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934, in connection with the Private Securities Litigation Reform Act of 1995. These forward-looking statements include, among others, statements regarding the potential effectiveness of Masimo Patient SafetyNet™. These forward-looking statements are based on current expectations about future events affecting us and are subject to risks and uncertainties, all of which are difficult to predict and many of which are beyond our control and could cause our actual results to differ materially and adversely from those expressed in our forward-looking statements as a result of various risk factors, including, but not limited to: risks related to our assumptions regarding the repeatability of clinical results; risks related to our belief that Masimo’s unique noninvasive measurement technologies, including Masimo Patient SafetyNet, contribute to positive clinical outcomes and patient safety; risks that Masimo Patient SafetyNet may fail to perform satisfactorily despite positive clinical evidence and its past success in UH; risks related to our belief that Masimo noninvasive medical breakthroughs provide cost-effective solutions and unique advantages; risks related to COVID-19; as well as other factors discussed in the “Risk Factors” section of our most recent reports filed with the Securities and Exchange Commission (“SEC”), which may be obtained for free at the SEC’s website at www.sec.gov. Although we believe that the expectations reflected in our forward-looking statements are reasonable, we do not know whether our expectations will prove correct. All forward-looking statements included in this press release are expressly qualified in their entirety by the foregoing cautionary statements. You are cautioned not to place undue reliance on these forward-looking statements, which speak only as of today’s date. We do not undertake any obligation to update, amend or clarify these statements or the “Risk Factors” contained in our most recent reports filed with the SEC, whether as a result of new information, future events or otherwise, except as may be required under the applicable securities laws.
Contacts
Masimo
Evan Lamb
949-396-3376
elamb@masimo.com
